11 Dec 2020
Introduction
Prone positioning is an intervention used in Acute Respiratory Distress Syndrome (ARDS) with the aim of improving oxygenation, preventing ventilator associated lung injury and, in combination with a protective ventilation strategy, has been shown to decrease mortality1. Placing the patient in the prone position is a strategy frequently undertaken for patients with COVID-19, particularly in mechanically ventilated patients during the first surge2.
Whilst there is little published evidence regarding enteral feeding in the prone position it has historically been thought to carry some risk of aspiration of gastric contents. In addition to the usual challenges of providing adequate nutrition in critically ill patients, feeding the patient in the prone position may pose an additional challenge due to decreased enteral feeding tolerance compared with patients in the supine position3.
As medical treatments for patients with COVID-19 evolve, prone positioning in awake patients is now increasingly undertaken. More recently, the ICS published guidance for ‘Prone Positioning of the Conscious COVID Patient, 2020’3. This recent guidance recommends 30 minutes to two hourly timed position changes for patients undergoing the ‘conscious prone position process’ with periods of ‘flat-bed positioning’. However, ICU’s may use different positioning techniques, with duration dependent on clinical need and resource.
Where evidence is lacking, recommendations have been based on the consensus of best practice by expert critical care dietitians within the British Dietetic Association CCSG and Critical Care Organisations.
Aims
The aims of this document are to:
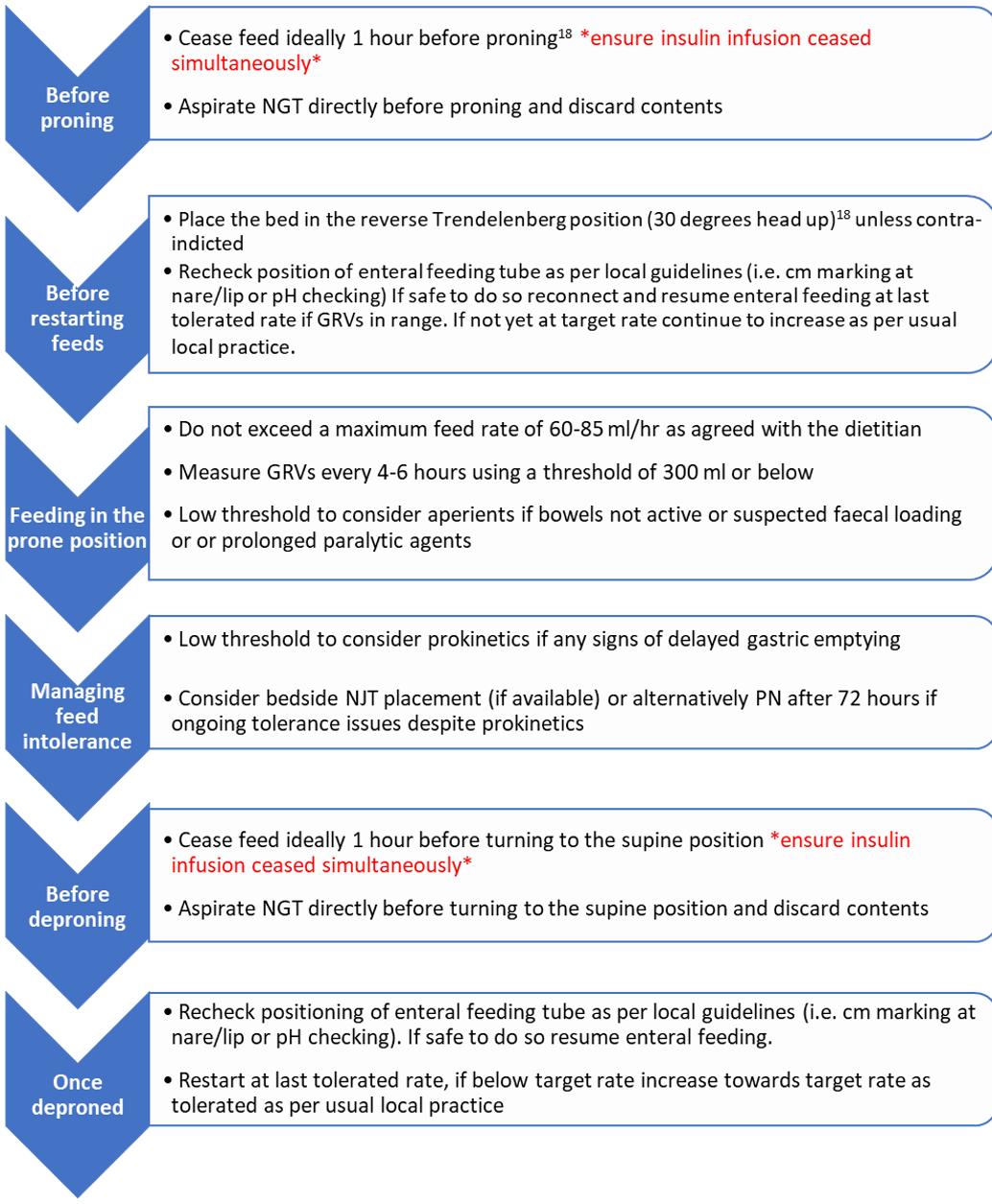
- Provide practical, pragmatic guidance to optimise nutrition and safe feeding in the prone position, for awake and sedated patients.
- Provide a summary of the evidence available.